HYPERACUSIS
HEARING DISORDERS
HYPERACUSIS
insidiously imprison
WHAT IS HYPERACUSIS
Firstly, it is important to refute the idea that the symptoms of hyperacusis are the manifestation of an auditory system affected by irreversible damage and that "you will have to live with it’ or ‘there is no solution", as is often claimed (except in specific cases defined by strict medical criteria).
Hyperacusis is a condition that affects the auditory system and is defined as an intolerance (rather than a heightened sensitivity to sounds) to environmental sound levels whose intensity, whether high or low, poses no risk or discomfort to people with normal hearing, but causes discomfort or physical pain in patients with hyperacusis. Hyperacusis is not synonymous with better hearing; hearing acuity is not improved.
For Natacha Chetritt-Bonneyrat, hyperacusis is a dysfunction of the auditory system caused by emotional trauma.
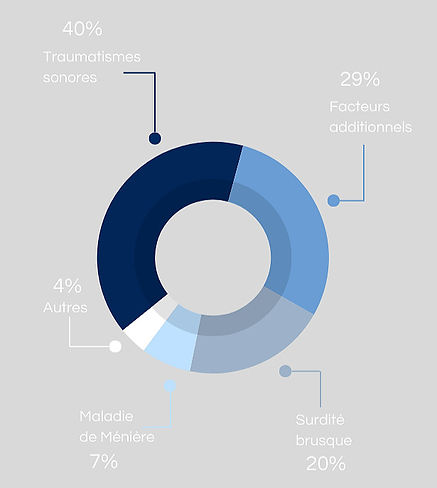
Hyperacusis is not always associated with hearing loss or other disorders affecting the auditory system, although statistically it is observed in 40%* of people with tinnitus (*source: France Acouphènes) and affects around 2% of the global population.
When symptoms of hyperacusis occur, whether or not they are associated with symptoms of tinnitus, it is medically impossible to predict whether we are dealing with a temporary episode or a phenomenon that will become permanent, giving rise to what we would describe as a ‘chronic disabling condition’.
It is common to see the first signs of hyperacusis appear 4 to 5 months after the onset of tinnitus symptoms.
Pathological auditory hypersensitivity results from the ear losing its functional dynamics, which manifests as a narrowing of the thresholds of discomfort and hearing: sounds of comfortable and loud intensity are exacerbated.
Audiométric Tests
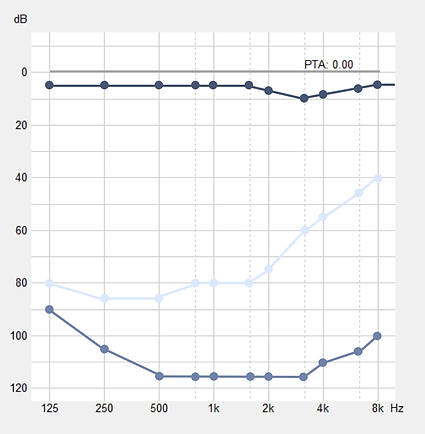
The following pattern hereinafter shows the main audiometric measures carried out by the medical team specialized in a patient affected by hyperacusis.
We notice that the values of the curve for tested thresholds of subjective discomfort are diminished when compared with those defined by the curve for reference thresholds of subjective discomfort (Fletcher’s Equal-Loudness Contours 115 dB).
The graph’s line for subjective discomfort thresholds measured in this patient has lost its typical concave form (banana or smile shape) from which results a more or less affected frequential range.
Consequently, and as most, this patient expresses a pain to certain sounds of lesser intensity whereas louder sounds only produce a moderate discomfort.
Represented in the graphic above, the corresponding values are :
Tonal audiometry reference point
Pure tone audiometry of the patient tested
Subjective discomfort threshold of tested patient
Subjective discomfort threshold reference point
WHAT ARE THE SYMPTOMS AND CONSEQUENCES OF HYPERACUSIS
Every illness requires medical attention. Only a doctor is qualified to diagnose. Thus, complementarity, openness, shared intelligence, offer better chances for healing than any isolated approach.
The symptoms which affect the hyperacusis patient are varied, without all of them necessarily manifesting at once.
.
Symptoms of hyperacusis
most commonly reported physical symptoms
- Hearing discomfort capable of reaching physical pain
- Clogged ears or fluffy sensation, hushed sound perception
- Tensing and snapping in the ear
- Warm auricle, sometimes with an exterior visible sign
- HeadachesNausea and dizziness
- Pain in the lower maxillary
- Acustics distortions
- Chronic fatigue
- Muscular tensions in other areas of the head or the nape of the neck
- Vibration feeling of the eardrum
Symptoms of hyperacusis
that are related to emotional disorders
- Loss of ‘joie de vivre’ (joy of life), “ life becomes dark, it loses meaning ”
- Behavioral issues " solitude, withdrawing into oneself, physical and mental seclusion ”
- Relationship hardships " the subject feels rejected, excluded, misunderstood by the medical profession and his/her close environment "
- Anxiety disorders and depressive state “ the subject sees himself/herself without any solutions, a lonesome path that many qualify as a descent into hell ”
- All communication becomes progressively difficult both in substance and in form
- Tendency to wall up in silence, to distance oneself from loved ones, desperately seeking a way to protect themselves from potential danger to come
- The person flees or endures, again and again, until exhaustion
- Behavior that can be perceived as obsessive by those around you
- Fear of having an irreversible pathology
In such cases, everyday benign noisy situations can then prove unbearable, such as: the noise of the shower jet hitting the tiles, the noise of scotch tape being rolled out, the noise of dishes clinking against each other, applauses, or high-pitched voices.
The sound of your own voice, the noise of your own feet and simply chewing can sometimes become intolerable.
Quantifying the pain is by no means proportional to the length of sound exposure; however exposure time may also be as detrimental as intensity.
Thus, the simple shout of a child can provoke a very strong pain that can last from a few hours to a few days.
Aware that the perception of certain sounds or the exposure to certain sound levels, even for a very short timespan, causes pain and fatigue, the hyperacusis patient will tend to protect himself/herself against any potential sound “attack” by wearing hearing protection (ear plugs) in most of everyday life situations.
In effect, hyperacusis concurs to a notable behavioral change in the affected subject, by setting up functioning patterns disproportionate to everyday situations.
It should be noted that hyperacusis does not fall under phonophobia, but that the legitimate protective attitudes of the hyperacusis patient can be the consequence of induced phonophobia.
It is frequently observed that one suffering from sound hypersensitivity sets up conditioned behavioral reflexes, without being aware of it, which considerably alter the quality of one’s everyday life and impact, up to the point of ruining it, one’s professional, personal and social life, thus affecting profoundly and lastingly one’s existence.
HOW TO DIAGNOSTIC AND TREAT HYPERACUSIS
Natacha Chetritt-Bonneyrat heals patients suffering from hyperacusis thanks to the alternative and intergrative approach of her tried and tested therapeutic protocol, during which the patient receives highly qualified personalized care.
An initial ‘preliminary assessment’ consultation is essential in order to diagnose and evaluate the symptoms of hyperacusis according to strict authorised medical tests and criteria. In addition, the ‘personal medical questionnaire’ completed by the patient is analysed to ensure that the ØREBLUE® therapeutic protocol is compatible with your condition and that all the necessary medical investigations have been carried out.
The ØREBLUE® therapeutic protocol eradicates completely and lastingly hyperacusis symptoms, as evidenced by the accounts of patients who have benefited from our therapy.
To date, the results observed in the treatment of hyperacusis are among the best in the world for patients who have scrupulously followed all of the recommended rehabilitation sessions, justified by their medical auditory and emotional profile. You can find these results by consulting the clinical study published in the medical journal Journal of Hearing Science.
Natacha Chetritt-Bonneyrat, through personal experience, is used to waiting until having observed a stable pathologic state of the subject (usually about 4 months after the apparition of the symptoms) before receiving the patient for the first appointment called the “Preliminary Checkup”.
This wisdom of time is primordial and must, despite granting time to first consult doctors in order to carry out the necessary researches, give time to nature to run its course and, if possible, offer a progressive and natural healing path.
During this first quadrimester, Natacha Chetritt-Bonneyrat has observed that hyperacusis symptoms are not mature, thus rendering any diagnosis unreliable, as to the severity of the symptoms and as to what appropriate care to give. She regrets the start of a hasty physiotherapy of the ear on a weakened auditory system, operated on by some, which, more often than not, disrupts a possible natural recovery.
On the other hand, it seems widely accepted that a psychological treatment by a seasoned health professional is often justified first off.
As many doctors have emphasized, without the patient’s determination to heal, the care provided, as exemplary as it may be, will be inefficient. The patient is the only architect of his own healing, with the practitioner’s guidance.
WHAT TO DO IF YOU HAVE HYPERACOUSIS
The appearance of a hyperacusis symptom, just like for tinnitus symptoms, is a matter of medical urgency and it is imperative to first consult the ENT specialist services under 48 hours.
Taking care of a person suffering from hyperacusis requires experience and much deftness.
When hyperacusis symptoms appear, associated or not to tinnitus symptoms, it is medically impossible to anticipate whether we are witnessing a temporary episode or a phenomenon that will set in durably to create what we will qualify as an " invalidating chronic pathology ”.
In this context, the patient suffering from hyperacusis must adopt a responsible and reasonable hearing hygiene by granting the necessary rest for one’s auditory system to “heal”: by removing all unnecessary sound solicitations from one’s daily life and by delegating as much as possible any task that would take one to noisy places (supermarkets, end of school days, professional meetings, restaurants, leisure activities…)
Wearing noise-reducing plugs will, temporarily and under certain conditions, be recommended to face certain unavoidable noisy situations. The goal, then, isn’t for the hyperacusis subject to have to handle every noisy situation indiscriminately and without preliminary caution, which would inevitably lead to the aggravation of the symptoms.
Using hearing protection must be done tactfully and moderately. Bearing this in mind, it is imperative to resort to custom-made plugs of the Pianissimo® type, the only ones to guarantee a linear filtration and to retitute he surrounding sounds faithfully. Any other protective hearing aid qualified as professional, even with superior noise reduction percentage, need to be proscribed.
In this situation, the hyperacusis patient must not, in any way, overprotect oneself in one’s daily life, which would increase one’s hypersensitivity.
CAUSES IDENTIFIED IN THE MANIFESTATION OF HYPERACOUSIS SYMPTOMS
Hyperacusis mostly appears following an acoustic trauma (concert, explosion, fire gun,…) or due to the repeated and extended exposure to high intensity sounds (music too loud, noisy working environment…)
However its sources of origin can be accidental (cranial trauma, ear barotrauma,…), the taking of ototoxic medicine, a psychological disorders such as PTSD (post-traumatic stress disorder), a sudden deafness, a viral affliction or still due to neurological confusions…
Less widespread, Bell’s facial paralysis, the Ramsay Hunt Syndrom (virus affecting neurons of the geniculate ganglion in charge of facial muscles’ movements, auricular herpes and facial paralysis), or a labyrinthine fistula can also concur to the appearance of hyperacusis symptoms.
More insidious, wearing noise-reducing plugs (ear plugs) in an inappropriate way to compensate an auditory discomfort or fatigue can induce the appearance of hyperacusis symptoms through the impoverishment of sensory stimuli.
This is just the concurrent visible reason, but we must never forget the “field” to use Pasteur’s words.